



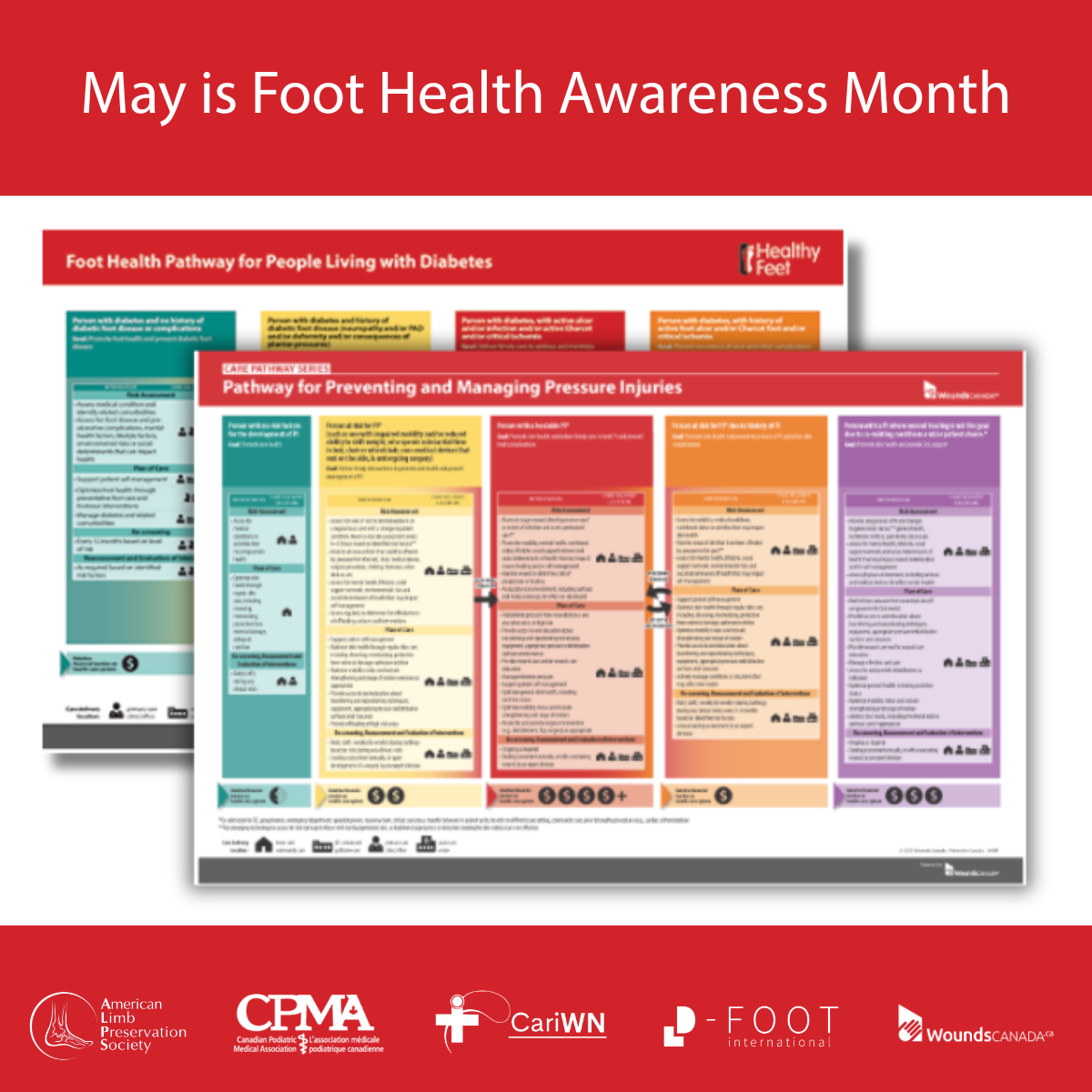



May is Foot Health Awareness Month. Help us spread awareness of healthy diabetic feet!
During the month of May, Wounds Canada is focusing on foot health, particularly for those who are living with diabetes. It’s important to know that diabetes increases risk for foot ulcers and other complications. There are several reasons for this. Among them:
- Loss of sensation because of nerve damage to the feet means the individual can’t feel discomfort or pain caused by external trauma, such as stepping on something sharp or developing a blister caused by shoes rubbing on the foot. This nerve damage is known as “neuropathy” and it can mean the person isn’t even aware that their foot has been damaged.
- Poor blood flow, also known as arterial insufficiency, can result in slow and/or incomplete healing for any damage that does occur.
- Poor vision is a consequence of diabetes that can make it difficult to inspect and care for feet properly.
All of these conditions can pose serious health risks—including ulcers, infections and even amputations—to a person’s feet. Current statistics show that 15–34% of patients with diabetes will develop a foot ulcer in their lifetime and that 80% of lower limb amputations are preceded by a diabetic foot ulcer. Yet, many are preventable through regular, consistent and purposeful action on the part of the person with diabetes, their family members and their health teams. In addition, they must be supported by health decision makers who set the policies to ensure best practice care in their regions.
Wounds Canada provides to all of these groups information, education and tools to keep the feet of all Canadians healthy.
This month join us in spreading awareness about foot health and the steps required to keep feet healthy and wound-free by amplifying our social media messages, talking to your friends and family about foot health and working with your health-care team to emphasize preventative action.
Whether you are a patient, clinician or policy maker you have a role to play in preventing diabetes-related amputations. This article outlines how everyone can work together to keep feet healthy in individuals with diabetes. Amputation Prevention: Your Role in Saving Limbs of Persons Living with Diabetic Foot Complications.
INTERVIEW WITH WOUND CARE INFLUENCER DR. MOHAMED MAGDY BADR ON DIABETIC FOOT PREVENTION AND ULCER TREATMENT
 With nearly 6000 followers on Linkedin, Dr. Mohamed Magdy Badr is a rising influencer in wound care. His lively illustrations cover current topics in the field with creativity, reaching a large audience. Badr is a physician in Cairo, Egypt, and a Wound Care Consultant at the Armed Forces Rehabilitation Center, Cairo, the Founder and CEO of Wound OnCall and a Geriatric Wound Care Specialist at Cairo Seniors Clinic. You can follow him online here.
With nearly 6000 followers on Linkedin, Dr. Mohamed Magdy Badr is a rising influencer in wound care. His lively illustrations cover current topics in the field with creativity, reaching a large audience. Badr is a physician in Cairo, Egypt, and a Wound Care Consultant at the Armed Forces Rehabilitation Center, Cairo, the Founder and CEO of Wound OnCall and a Geriatric Wound Care Specialist at Cairo Seniors Clinic. You can follow him online here.
WC: How do socioeconomic inequalities influence diabetic foot outcomes even before “high-risk” classification develops?
Socioeconomic inequality is one of the most underestimated drivers of diabetic foot complications. Many patients are classified clinically as “low risk,” yet they live in environments that expose them to high practical risk. Limited income may affect their ability to buy protective footwear, attend follow-up visits, access early vascular assessment, or even take time off work when early symptoms appear. A patient may not have neuropathy today, but if they walk long distances in poor footwear, delay care because of cost and lack health education, their real-world risk is already elevated. This is why diabetic foot prevention should not rely only on biological risk factors. It should also include social risk factors such as affordability, occupation, distance from care, education level and family support.
WC: Are current health-care systems too focused on ulcer treatment rather than mobility preservation?
Yes. Many systems still define success as wound closure, but wound closure alone is not enough. A healed ulcer over an unstable foot, poor footwear, persistent deformity, or unresolved ischemia is not true success. It is often only a temporary pause before recurrence. The real goal should be mobility preservation.
This means we should ask:
• Can the patient walk safely?
• Can they return to work?
• Can they wear appropriate footwear?
• Has pressure been redistributed?
• Has recurrence risk been reduced?
• Has the patient regained confidence?
Diabetic foot care should move from a “wound-centred model” to a “function-centred model.”
WC: How can wearable technology and AI reshape early detection of tissue stress before ulceration occurs?
Wearable technology and AI may become major tools in diabetic foot prevention. Many ulcers are not sudden events. They are the final stage of repeated pressure, heat, friction, inflammation and unnoticed tissue stress.
Wearables can help detect:
• Abnormal plantar pressure
• Temperature differences between feet
• Reduced activity or altered gait
• Repetitive stress points
• Early inflammation before skin breakdown
AI can combine these signals with clinical history, footwear data, vascular status, neuropathy status and previous wound history to create a personalized risk profile.
WC: What role does patient psychology play in delayed presentation and poor adherence?
Patient psychology is central. Many patients do not ignore advice because they are careless. They may be afraid, overwhelmed, in denial, embarrassed, financially stressed or simply unable to connect daily foot care with future limb loss.
Common psychological barriers include:
• Low perceived risk
• Fear of diagnosis
• Denial of diabetes complications
• Treatment fatigue
• Depression
• Previous negative healthcare experiences
• Belief that “small wounds heal by themselves”
This is why education should not be delivered as instruction only. It should be delivered as behavior change support. We need empathy, repetition, motivational interviewing, simple routines, family engagement and emotionally meaningful messages. The future is not only detecting ulcers early. The future is detecting pre-ulcerative stress before the wound exists.
WC: Should diabetic foot prevention begin at the diagnosis of diabetes itself rather than after neuropathy develops?
Yes, absolutely. Waiting for neuropathy before starting prevention is like waiting for brake failure before teaching safe driving. The moment diabetes is diagnosed, patients should understand that the foot is a lifelong target organ of diabetes.
Early prevention should include:
• Foot hygiene
• Nail care
• Shoe selection
• Avoiding barefoot walking
• Skin moisturizing
• Early reporting of redness, swelling, blisters, callus, or wounds
• Understanding the danger of minor trauma
The goal is to build habits before complications appear, not after.
WC: How can digital education, social media, and visual storytelling improve preventive behaviors in younger generations?
Younger patients often respond better to short, visual, repeated messages than traditional clinic leaflets. Digital education can deliver prevention through:
• Short videos
• Infographics
• WhatsApp reminders
• Social media posts
• Patient stories
• Visual warning signs
• Interactive quizzes
• AI-based personalized education
The message must be simple, frequent, emotional and visually memorable. For example, instead of saying: “Inspect your feet daily,” we can say: “Your foot may be injured before it hurts. Look before you walk.” This type of message is easier to remember and more likely to change behavior.
WC: What lessons from military rehabilitation systems can civilian diabetic foot programs adopt?
Military rehabilitation often focuses strongly on function, performance, teamwork and reintegration. Civilian diabetic foot programs can learn several principles:
• Early multidisciplinary involvement
• Clear rehabilitation goals from day one
• Psychological support as part of physical recovery
• Prosthetic and orthotic integration
• Functional outcome measurement
• Return-to-role planning
• Team-based case conferences
The military model reminds us that healing is not the end. Return to function is the mission.
Illustration by Dr. Mohamed Magdy Badr




